If you buy, secure, or maintain medical devices, you now need SBOM rules in place. In U.S. healthcare, software risk is tied to patient care, FDA review, vendor contracts, and HIPAA duties.
Here’s the short version:
- FDA Section 524B lets the FDA reject premarket submissions for cyber devices that do not include an SBOM.
- Medical devices often contain 75% to 80% third-party code, which makes software risk hard to track without vendor disclosure.
- Large hospitals may manage 10,000 to 15,000 connected devices, so manual checks do not scale.
- HIPAA penalties can reach $2,134,831 per violation per year as of 2025.
- A usable SBOM should include more than a parts list: it should have versions, dependencies, support status, EOS/EOL dates, and VEX data.
- If I were setting policy today, I would require machine-readable SBOMs, updates with every software change, and contract terms that let me reject incomplete disclosures.
What matters most is simple: you need to know what software is inside your devices, whether a flaw affects you, and who is responsible for acting on it.
Webinar: Managing Compliance with the FDA's SBOM Requirements
Quick comparison
| Area | What I’d look for |
|---|---|
| Regulation | FDA 524B SBOM support for cyber devices |
| Minimum content | NTIA fields: supplier, component, version, identifier, dependency, author, timestamp |
| Format | CycloneDX or SPDX |
| Extra detail | Full dependency tree, CPE/PURL, support status, EOS/EOL |
| Vulnerability context | VEX plus CVE and CISA KEV checks |
| Delivery | At purchase and after every patch or dependency change |
| Governance | Security, clinical engineering, procurement, and compliance each own part of the process |
| Procurement rule | No SBOM, no approval for in-scope devices |
I’d treat SBOM disclosure as a clear business rule, not just a security task. It helps you cut vendor back-and-forth, sort device exposure faster, and document risk in a way regulators and internal teams can follow.
The U.S. Regulatory and Standards Landscape for SBOM Disclosure
FDA Section 524B Requirements for Cyber Devices
Section 524B of the FD&C Act says manufacturers of FDA-defined cyber devices must include an SBOM in every premarket submission. A device counts as a cyber device if it contains software or firmware, can connect to a network or the internet either directly or indirectly, and has traits that a cybersecurity threat could exploit [6][2].
The FDA wants more than a plain parts list. For each component, it expects lifecycle metadata such as support level, end-of-support dates, known CVEs, CISA KEV matches, and mitigation plans [2][7]. It also asks more often for VEX files alongside SBOMs so reviewers can see whether a given vulnerability is exploitable in the device’s actual setup [2].
This matters in practice. Cybersecurity deficiencies, including incomplete SBOMs, are one of the main reasons the FDA sends "Additional Information" requests during 510(k) and PMA reviews [7]. And when a patch lands or a dependency changes, the SBOM should be updated and versioned across the device lifecycle [2][7].
That legal baseline shapes what healthcare organizations should ask for during procurement.
NTIA, CISA, NIST, and IMDRF Guidance on SBOMs
The FDA isn’t working alone here. Other agencies and standards groups have helped spell out what a usable SBOM should include.
NTIA’s minimum elements set the starting point:
- Supplier Name
- Component Name
- Version String
- Unique Identifier
- Dependency Relationship
- SBOM Author
- Timestamp [2][5]
For devices with more risk, the FDA may also want end-to-end documentation, including the build tools and toolchains used during compilation [7].
CISA and NIST add the day-to-day security angle. CISA’s KEV catalog lets teams check SBOM components against flaws that attackers are actively using. NIST’s cybersecurity framework helps fold SBOM data into broader risk management and vulnerability triage work. IMDRF N73, published in 2023, pushes the same direction at the global level and recommends that manufacturers share SBOMs with healthcare providers to support internal risk management across the full device lifecycle [2].
These groups set the floor. The harder part is turning that into disclosure terms people can actually use.
| Framework | Role in SBOM Disclosure |
|---|---|
| FDA Section 524B | Legal mandate for cyber devices; SBOMs required in premarket submissions |
| NTIA Minimum Elements | Seven baseline data fields required in any compliant SBOM |
| CISA KEV Catalog | Cross-reference tool for identifying actively exploited component vulnerabilities |
| NIST Cybersecurity Framework | Integrates SBOM use into enterprise cybersecurity risk management practices |
| IMDRF N73 | International best-practice principles for SBOM sharing across the device lifecycle |
| VEX | Companion document clarifying whether a known vulnerability is exploitable in a specific device |
On file format, the FDA accepts SPDX, CycloneDX, and SWID. CycloneDX is often a strong match for security-focused healthcare teams because it supports VEX natively and fits security workflows well [2][7].
Contract, Procurement, and Disclosure Obligations Beyond Regulation
Federal rules set the minimum. Contracts are where SBOM terms usually get sharp and specific. More healthcare organizations now put SBOM requirements straight into purchasing agreements and vendor due diligence, long before a device ever reaches the floor [2].
A supplier contract should spell out three points clearly:
- Delivery timing: require SBOMs at purchase and with every later software release.
- Update frequency: require SBOM delivery with every patch or dependency change, not just the first shipment.
- VEX support: require VEX so teams can tell the difference between exploitable and non-exploitable vulnerabilities [2].
"SBOMs exist to make that supply chain transparent... just as food packaging lists every ingredient, an SBOM lists every software component." - Ran Chen, Global MedTech Expert [2]
SBOMs are also being tied more closely to ISO 13485 configuration management practices. In plain terms, they should connect to a device’s change-control workflows and Device Master Record. That link matters during post-market surveillance, when a hospital or health system needs to trace a reported safety or security event back to a specific software component version [2].
Write SBOM delivery, update, and VEX terms into contracts before purchase. Those terms shape how fast your team can review, compare, and act on SBOM data.
sbb-itb-535baee
What Healthcare Organizations Should Expect in an SBOM Disclosure
Minimum Data Fields and Quality Indicators
Once the disclosure rules are clear, the next issue is simple: what makes an SBOM usable day to day?
Compliance by itself doesn't get you there. NTIA fields are the starting point. A usable SBOM gives security, procurement, and clinical engineering the detail they need to review software risk before and after purchase.
Go past the baseline. Ask for SBOMs that are machine-readable, digitally signed, and include the full dependency tree, including nested dependencies. Each component should also include lifecycle details, such as support status, End-of-Support (EOS), and End-of-Life (EOL) dates.
Versionless component names don't help much with vulnerability review. Most medical device software relies heavily on third-party code, so version strings and PURL or CPE identifiers matter. Without them, it's hard to match components against vulnerability sources like the NVD or CISA KEV.
Ask for VEX alongside the SBOM. That helps teams sort exploitable vulnerabilities from non-exploitable ones and cuts down false positives during intake.
Formats, Granularity, and Delivery Methods
Format can make or break whether teams can use the SBOM at all.
Accept SPDX or CycloneDX in machine-readable form. Also require a delivery method that supports updates after each release. An SBOM that arrives once and never changes won't help much after patches or dependency shifts.
The market is moving away from static email attachments and toward web portals, customer-facing APIs, and direct-to-integrator feeds. When you assess a manufacturer, ask how SBOM updates are delivered after a patch or dependency change. That detail matters because security, procurement, and clinical engineering need data they can ingest without manual cleanup.
How to Use SBOMs in Procurement and Device Evaluation
An SBOM reviewed before purchase can surface problems that become expensive once a device is already on the floor.
Watch for unsupported or abandoned components. Libraries that no longer receive security patches create an ongoing liability. Legacy dependencies that haven't been replaced can quietly become your maintenance burden.
SBOMs can also show patching limits. Some medical device architectures make it hard - or impossible - to update single components without a full firmware release. If you know that before purchase, your team can plan for patching timelines that match reality and put compensating controls in place, such as network segmentation.
Tie SBOM review straight to total cost of ownership. A device may look competitively priced at acquisition but still bring hidden costs if its software stack depends on components nearing end-of-life.
A practical way to handle review:
- Use full dependency trees and build-tool inventories for high-risk devices.
- Use a complete top-level component list for lower-risk assets.
- Reject incomplete SBOMs at intake.
The next step is moving SBOMs from procurement review into ongoing risk operations.
Putting SBOMs to Work Across Risk, Security, and Clinical Workflows
Governance and Ownership Across Security, Clinical Engineering, and Supply Chain
An SBOM only helps if someone owns it and knows what to do next. It needs to connect to the teams that can triage issues, patch systems, isolate devices, and document risk.
In practice, that means each group has a clear role. Cybersecurity and CISO teams handle vulnerability triage, component reachability, and incident response when new CVEs show up. Clinical engineering manages patch windows, asset mapping, and compensating controls. Procurement and supply chain teams enforce SBOM delivery clauses and acceptance rules. Legal and compliance teams build SBOM delivery and notification terms into vendor agreements.
The smartest move is to plug SBOM work into existing risk committees and cyber risk processes instead of building a separate track. That matters most when a new vulnerability appears and teams need to move fast with a clear, documented response.
Once ownership is set, SBOMs can guide triage, patching, and procurement decisions.
Using SBOMs for Vulnerability Triage and Incident Response
Governance falls apart if SBOMs don't feed day-to-day response. Disclosure only helps when teams can match it to live assets and current threats. When a new CVE or KEV item appears, SBOMs help answer the first question fast: is this component in use?
A standard response matrix keeps triage consistent.
| SBOM Finding | Action | Primary Owner | Priority |
|---|---|---|---|
| New CVE in CISA KEV | Immediate triage; determine exploitability via VEX or exploit-path analysis | CISO / Security Ops | High (24–72 hours) |
| Critical CVE (Critical Internet-Facing) | Patch or isolate within 14 days | IT / Security | High |
| Critical CVE (Internal/Clinical) | Patch within 30 days or next maintenance window; apply network segmentation if patch requires full firmware release | Clinical Engineering | Medium |
| Non-Exploitable CVE (per VEX) | Document "not affected" status in risk file; no patch required | Security / Compliance | Low |
| End-of-Life Component | Evaluate replacement roadmap or long-term isolation strategy | Procurement / IT | Medium |
| New Procurement (Missing SBOM) | Reject delivery or hold payment | Procurement / Legal | High |
If patching is blocked, the focus shifts. Teams move to isolation, monitoring, and replacement planning.
Scaling SBOM Management with Healthcare-Focused Risk Operations
The same process still has to work across thousands of devices. At that point, manual SBOM tracking starts to break down.
Healthcare leaders need one central workflow for SBOM findings, vendor risk, and remediation. Censinet RiskOps™ supports that by linking SBOM findings, vendor assessments, and remediation tasks across security and clinical stakeholders [4].
The aim is one operational view of SBOM findings, vendor risk, and remediation - supporting compliance, resilience, and patient safety across the enterprise.
A Practical Maturity Roadmap for Healthcare Leaders
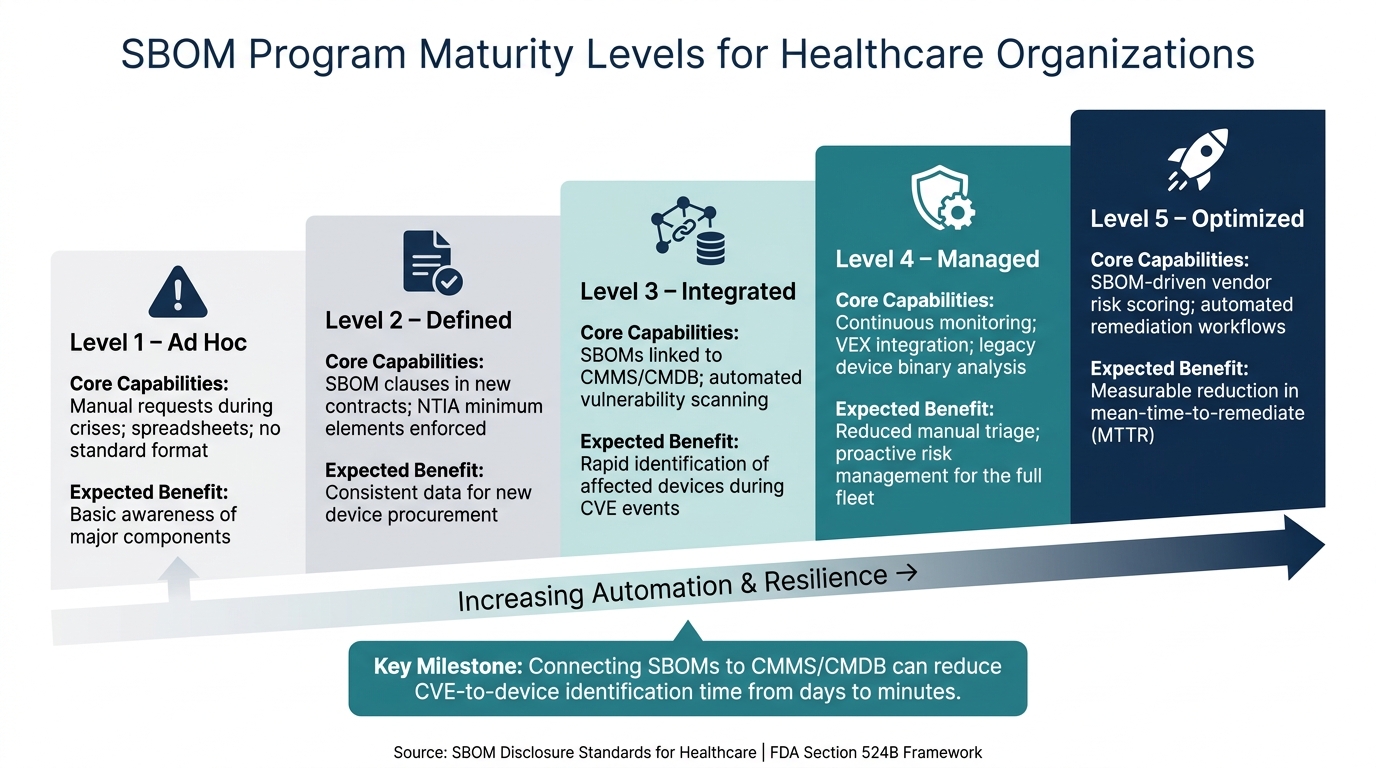
SBOM Maturity Levels for Healthcare Organizations
Once SBOMs start helping with triage and procurement, the next hurdle is scale.
Maturity Stages: From Ad Hoc Requests to an Integrated SBOM Program
Most healthcare organizations begin with ad hoc SBOM requests and spreadsheets. That may work for a while, but it falls apart once the device count grows. [3] The stages below show how teams move from manual intake to an automated response model.
| Maturity Level | Core Capabilities | Expected Benefits |
|---|---|---|
| Level 1: Ad Hoc | Manual requests during crises; spreadsheets; no standard format | Basic awareness of major components |
| Level 2: Defined | SBOM clauses in new contracts; NTIA minimum elements enforced | Consistent data for new device procurement |
| Level 3: Integrated | SBOMs linked to CMMS/CMDB; automated vulnerability scanning | Rapid identification of affected devices during CVE events |
| Level 4: Managed | Continuous monitoring; VEX integration; legacy device binary analysis | Reduced manual triage; proactive risk management for the full fleet |
| Level 5: Optimized | SBOM-driven vendor risk scoring; automated remediation workflows | Measurable reduction in mean-time-to-remediate (MTTR) |
The biggest jump happens when SBOMs connect to asset records and vulnerability workflows. Once SBOMs are tied to your CMMS or CMDB, finding the physical devices affected by a new CVE can drop from days to minutes. [3]
Priority Actions for the Next 12 to 24 Months
Over the next 12 to 24 months, the focus should be clear: tighten procurement controls, map assets, and automate response.
Start with contracts. Add SBOM delivery terms to new procurement agreements. Ask for machine-readable SBOMs in CycloneDX or SPDX format, with transitive dependencies and version details included. [3]
Connect SBOMs to your asset records. Map ingested SBOM data straight into your CMMS or CMDB. Then, when a new issue appears in the CISA Known Exploited Vulnerabilities (KEV) Catalog, your team can quickly see which devices are exposed. [3]
Set a clear baseline for acceptance. Use the NTIA Minimum Elements as the floor. [1][2] If an SBOM is incomplete, treat that as a procurement failure.
Ask for VEX with every SBOM. That gives teams a way to sort exploitable findings from noise. [2]
For legacy devices, things get messier. If manufacturers can’t provide SBOMs, put binary analysis first on the equipment with the highest risk and the most exposure. [3]
Conclusion: Key Takeaways for Compliance, Resilience, and Patient Safety
SBOM disclosure is now both a regulatory and contract issue. FDA Section 524B made SBOMs a legal requirement for cyber devices as of October 1, 2023, and procurement teams across U.S. healthcare are more and more treating them as a hard gate, not an optional deliverable. [2][3]
Format and delivery still matter. But quality and update cadence matter even more. Teams need version-level detail because component names alone don’t give enough information for vulnerability assessment. The bar has to sit above the minimum.
Turning disclosure into action takes governance and the right operational setup. Centralized risk workflows help teams move from SBOM paperwork to faster remediation and safer care.
FAQs
Which devices need an SBOM?
Under U.S. rules, an SBOM is legally required for cyber devices. That means devices that include software, can connect to a network or the internet, and have features that could be exposed to cybersecurity threats.
For other software-based medical devices, an SBOM isn't legally required. Still, the FDA strongly recommends one because it helps with transparency and risk management.
What makes an SBOM usable?
An SBOM becomes useful when it goes beyond a static list. It should be a machine-readable inventory that teams can actually use for active risk management.
For that to work, the SBOM needs full version details, transitive dependencies, and standard identifiers. In healthcare, it also needs to fit into day-to-day workflows that check data quality, watch for vulnerabilities on a continuous basis, and rank fixes based on clinical context and exploitability.
How should hospitals handle missing SBOMs?
Hospitals should start by asking the manufacturer for the SBOM. Some vendors will share it on request, even for older products.
If the SBOM isn’t available, hospitals can turn to binary analysis tools to build an approximate list of components. From there, they can put compensating controls in place to protect high-priority clinical assets, including:
- Network segmentation
- Monitoring
- Access restrictions
